Cavities are one of the most common dental problems, but thanks to modern materials, fixing them doesn’t mean compromising the look of your smile. At Luka Dental Care in London, ON, we use natural-looking composite fillings that blend in seamlessly with your teeth while restoring strength and function.
Whether you’ve just discovered a new cavity or need to replace an old silver filling, we’ll make the process comfortable, efficient, and customized to your needs.
Composite fillings are tooth-colored restorations used to treat small to medium areas of decay. Made from a blend of resin and finely ground glass, these fillings are designed to match the natural shade of your enamel, making them practically invisible once placed.
They’re an excellent alternative to traditional silver (amalgam) fillings, especially for patients who want a more aesthetic option or are concerned about metal in their mouths.

While amalgam fillings were once the gold standard, composite materials have come a long way. Today’s composites are durable, versatile, and much more attractive.
Benefits of composite fillings:

Blends in naturally with your existing tooth structure
Preserves more healthy tooth during placement
Bonds directly to the tooth, adding strength and support
Mercury-free and metal-free
Ideal for front and back teeth
Because composite fillings bond chemically to your enamel, they often require less drilling than amalgam fillings. That means more of your natural tooth stays intact—and you get a restoration that functions well and looks great.
Fillings are primarily used to treat cavities, but they also serve several other restorative purposes. At Luka Dental Care in London, ON, we may recommend a composite filling for:
Treating tooth decay caused by bacteria and plaque
Repairing chipped or worn teeth
Reshaping a misshapen tooth for cosmetic reasons
Replacing old or cracked metal fillings
Sealing a minor crack or fracture
No matter the reason, composite material allows us to restore form and function while keeping your smile looking natural.
Not all cavities cause pain—some can exist for months without noticeable symptoms. That’s why regular checkups at our London dental office are so important. During your visit, we’ll use digital X-rays and intraoral imaging to look for any signs of decay or damage that may not be visible to the eye.
You might need a filling if you experience:





Getting a filling at Luka Dental Care is a quick and comfortable experience. Here’s how the process works:
We apply local anesthesia to the area to ensure you don’t feel any pain during the procedure.
We gently remove the decayed portion of the tooth using precise instruments.
We clean and shape the cavity to prepare it for bonding.
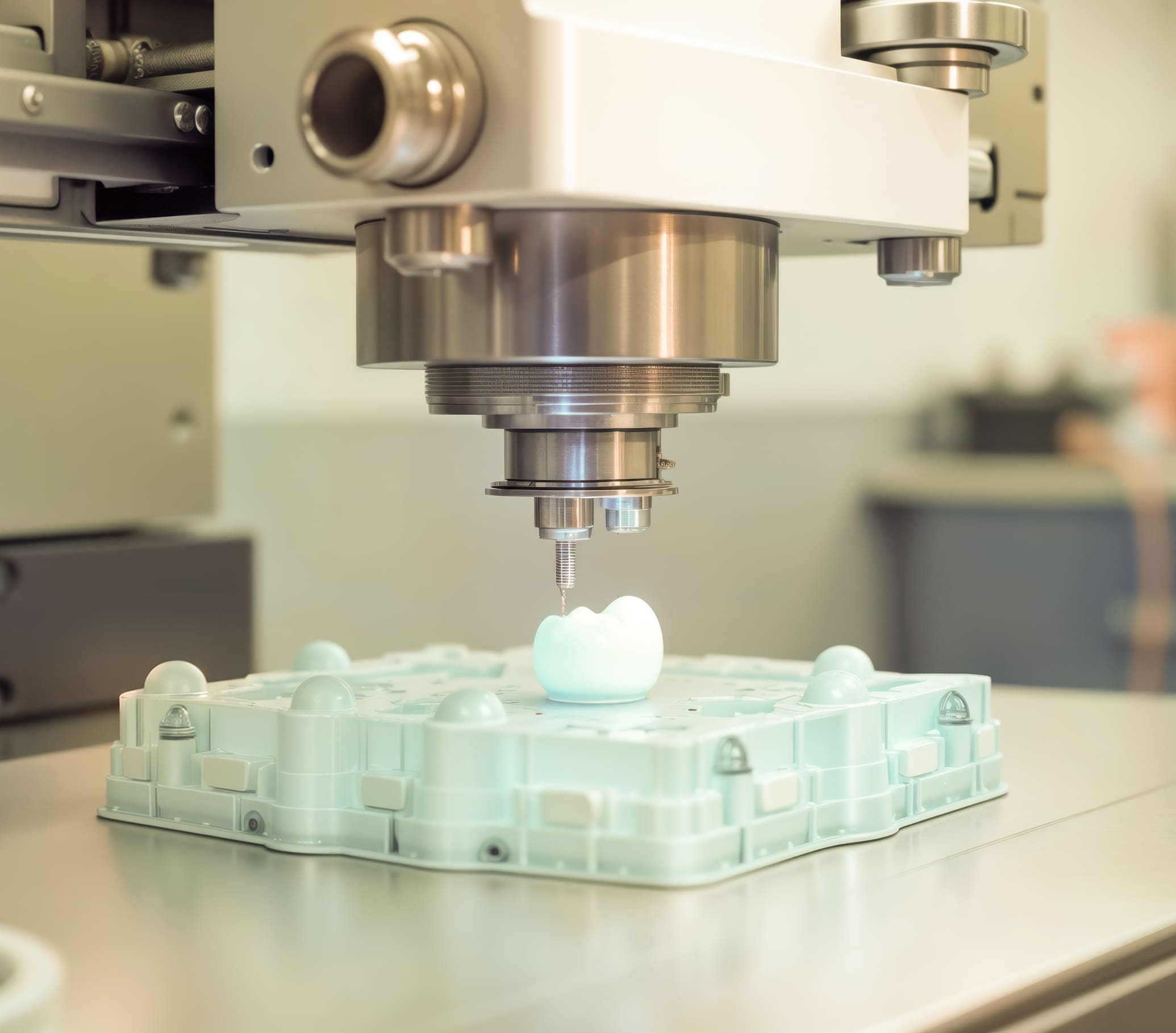
The composite resin is layered into the cavity and hardened using a special curing light.
We sculpt and polish the filling so it feels smooth and matches your bite.
Most fillings are completed in under an hour, and you can return to your normal routine immediately afterward.
Composite fillings do more than just “fill” a cavity—they restore the integrity of your tooth in a way that’s functional, comfortable, and cosmetically appealing.
Aesthetically superior
No one will know you’ve had dental work done
Strong and supportive
Bonds to the tooth to help prevent future fractures
Minimal drilling required
More natural tooth structure is preserved
No temperature sensitivity from metal
Long-lasting when properly cared for (7–10+ years)
We use the latest tools and techniques to make your filling experience as smooth and effective as possible.

Reveal decay between teeth and under existing restorations
Help us show you exactly where the issue is

Selected for strength, longevity, and aesthetics
Ensures your filling blends perfectly with surrounding enamel
Composite fillings are a great solution for existing decay—but prevention is always better. We’ll equip you with practical habits to lower your cavity risk: brush twice daily with fluoride toothpaste, floss every day, limit sugary drinks and snacks, book professional exams and cleanings every six months, and consider fluoride treatments or sealants if you’re prone to decay.
The better your daily routine, the fewer fillings you’ll need—and the longer your restorations will last.
Over time, even the most durable dental materials can begin to wear down. Metal fillings may corrode or develop microscopic cracks, allowing bacteria to seep underneath and cause hidden decay.
At Luka Dental Care in London, we carefully assess your existing fillings for signs of marginal breakdown, recurrent decay, tooth discoloration or sensitivity, and surface cracks or structural damage. Identifying these issues early can help prevent more serious problems down the line.
If replacement is needed, we’ll remove the old material and restore the tooth with a modern composite filling that’s safer, stronger, and far more natural-looking. It’s a simple upgrade that can make a big difference in both your oral health and your confidence.

While composite fillings are ideal for most cases, they’re not always the best solution. In some situations—like very large cavities or teeth that bear heavy biting forces—we may recommend an alternative, such as an inlay, onlay, or dental crown.
We might suggest something other than composite if:
In every case, we’ll walk you through your options and help you choose the solution that offers the best balance of durability, aesthetics, and long-term health.

Brian K.
Luka Dental Care Patient

We don’t just treat teeth—we care for people. Our approach to composite fillings is grounded in skill, comfort, and clear communication. We take the time to explain your options, answer your questions, and ensure you feel completely at ease before, during, and after your visit.
What sets us apart:

Your restorations will look and feel natural

We move at your pace and use gentle techniques

We take time to do it right—and make sure you’re comfortable
If you have a cavity, damaged filling, or just want a more natural alternative to metal, we’re here to help you in London, Ontario. Composite fillings at Luka Dental Care are fast, effective, and designed to blend seamlessly with your smile.
On average, 7 to 10 years—but with good brushing, flossing, and regular checkups, they can last even longer.
Yes. They are biocompatible, free of mercury, and have been used successfully in dentistry for decades.
We use local anesthetic to numb the area, and most patients feel little to no discomfort during or after the procedure.
Yes! Many patients choose to replace old silver fillings for aesthetic reasons or due to wear. We’ll let you know if yours should be upgraded.
They’re more stain-resistant than natural enamel but can darken slightly over time with exposure to coffee, tea, or smoking.
Yes. Composite fillings are cured instantly with light. You can eat as soon as the numbing wears off—though we recommend starting with soft foods.
Yes, some sensitivity to pressure or temperature is common for a few days, especially if the cavity was deep. It should fade within a week or two. If not, let us know so we can check the bite or consider other solutions.
You may notice sensitivity, roughness, discoloration, or a feeling that something is off. But the most reliable way is to visit us for a checkup—we can assess it with visual inspection, X-rays, and testing.
It’s rare, but it can happen if the bonding fails or the tooth fractures. If a filling comes loose or falls out, call us as soon as possible so we can restore the tooth and prevent further damage.

2101 Aldersbrook Rd, London, ON N6G 3X1